
AA is a merger of cauda equina nerve roots and the arachnoid lining of the spinal canal covering which forms an inflammatory mass or clump that entraps nerve roots.
ANATOMIC LOCATION: The definition above is applicable to the most common location of AA which is the lumbar-sacral spine. On very rare occasions the spinal cord or brain can merge with the arachnoid lining of the spinal cover of the spinal canal or brain (meninges).

PHYSIOLOGIC EFFECT
The gluing of cauda equina nerve roots and the arachnoid lining form an inflammatory, adhesive mass or clump that entraps nerves. The mass may erode through the entire spinal canal cover (arachnoid and dura) and cause spinal fluid to leak into tissues between the spine and skin over the lower back. The mass causes intense pain, nerve root dysfunction, and interferes with spinal fluid flow which causes symptoms including headache, blurred vision, dizziness, ringing in ears, and poor balance.
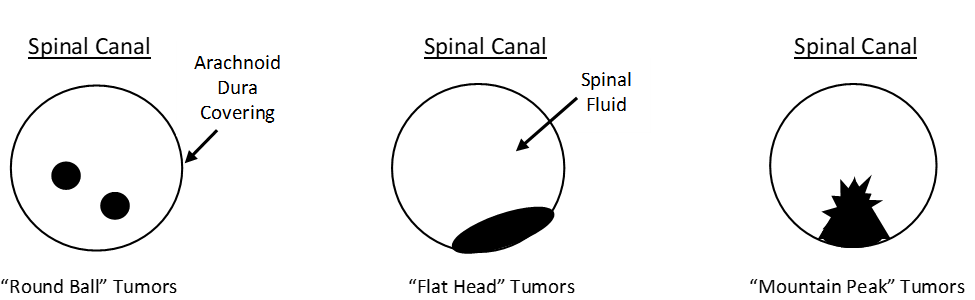
There are three basic tumor types:
ADHESIVE ARACHNOIDITIS (AA) IS THE END STAGE OF INTRASPINAL CANAL INFLAMMATION
In our Arachnoiditis Research & Education Project we have reviewed the MRI’s of over 300 persons with the typical symptom profile of AA which includes back pain, stabbing pains, sensations of insects/water on the skin, leg weakness, pain relief on reclining or standing, blurred vision, and urinary dysfunction.
MAJOR DISCOVERY: Many persons with the symptom profile of AA do not show the diagnostic sign of cauda equina nerve root clumping or coalescence that is necessary for the diagnosis of AA. The MRI will, however, almost always show some anatomic abnormalities of the nerve roots including enlargement, loss of circular contour, or displacement from their normal symmetrical pattern.
THE INTRASPINAL INFLAMMATORY PROCESS: Persons with AA are the end result of intraspinal canal inflammation that may take months or years to cause the formation of adhesions and clumping that will show as AA on MRI. Symptoms begin with the initiation of inflammation. Inflammatory markers may elevate in the blood. Aggressive suppression of intraspinal canal inflammation is necessary to prevent AA.
THE INTRASPINAL INFLAMMATION PROCESS:

CONCLUSIONS:
- Many persons with intraspinal canal inflammation develop the symptom profile of AA, but the diagnostic clumping of nerve roots which is necessary for a diagnosis of AA may not be evident.
- Intraspinal canal inflammation may show non-clumping evidence on an MRI and elevated inflammation markers in the blood.
- Aggressive anti-intraspinal canal inflammatory treatment should be initiated as soon as possible to prevent AA.